

How To Reduce Thick Skin On Nose
Abstract
Aesthetic correction of a big olfactory organ, especially in the instance of thick spongy skin, is always connected with some difficulties, because of unpredictable results of the corrective intervention.
Purpose: To present open rhinoplasty technique modification when nosotros remove nose skin excess with post-operative cicatrices in barely visible places.
Material and methods: The main techniques that nosotros used while performing aesthetic rhinoplasty, with excision of peel excess included, were the following:
1. Original marking of the surgical intervention area.
2. Incisions and extensive mobilization of the nose cutaneous covering.
3. Necessary correction of the nose base back up structures, especially of the nasal tip and olfactory organ wings.
4. Excess nose skin removal, with mail service-operative cicatrices in barely visible places.
Results: We accept used this surgery technique since 2002 in 48 cases. By and large the results obtained were characterized as practiced and satisfactory.
Conclusions: The mentioned modification of open up rhinoplasty can be effective in the case of rhinomegaly, when there is a sufficient backlog of thick porous skin and rounded or long nasal tip and nostrils.
Key words
rhinoplasty, rhinomegaly, big olfactory organ, nose pare excess
Introduction
From a large diverseness of external nose aesthetic deformations, big noses with thick porous skin are e'er operated on very unwillingly even past experienced rhinologists [1-9].
Here are the reasons
Thick porous skin does not contract properly during the mail service-operative period. It does non conform to the position of the support frameworks. That is why the nose frequently takes shapeless contours (Figure one).

Effigy one. The example of complications after close rhinoplasty that happened while operating on the patient with a thick, porous skin – shapeless nasal tip, dimension mismatch of the cartilaginous stractures and skin.
Cutaneous covering excess on the nasal tip, nasal arch, lateral nasal walls, and wings of the olfactory organ, that sometimes appear after the nose support structures reduction, should be excised. However, today just the method of shortening the nose length and decreasing of the nasal wings convexity with post-operative cicatrices in barely visible places is offered. Information technology is not always enough for getting practiced results. And aesthetically open-door ways of excess skin removal from the other parts of the nose exercise not exist. Surgeons have to perform skin resections in visible parts of the nose (Figures 2, 2a, and 2b) [1-5]. These methods do non take their followers considering of the possibility of getting postal service-operative cicatrices on the aesthetically important olfactory organ parts. We either have never practiced such incisions or pare resections during rhinoplasty, although we oftentimes have faced the necessity of using them [6].

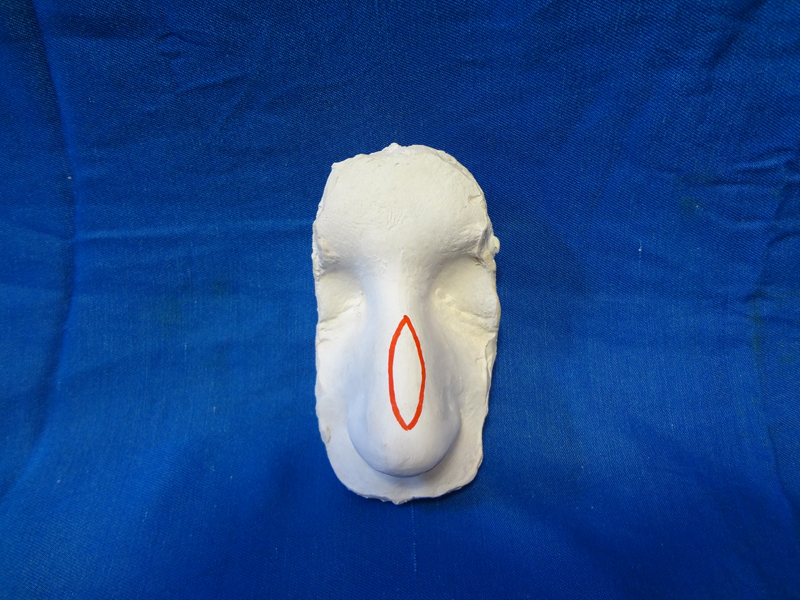
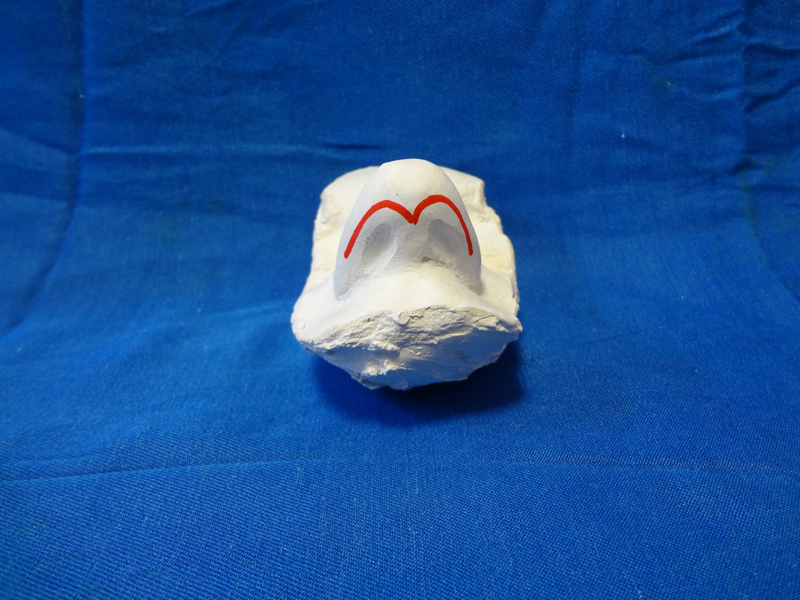
Figure 2, 2a, 2b. Plaster casts on which yous can see incision marker for excess skin excisions – classical variants.
For that very reason in 2002 we developed such a modification of rhinoplasty that enabled us to excise pare excess using incisions in barely visible parts of the nose [7-9].
The purpose
The purpose is to present the method of excess nose pare removal from the nose during rhinoplasty, that could make it possible "to hide" post-operative cicatrices in barely visible places. Meanwhile, we focused our attention on the noses that were supposed to become reduction of the nasal tip skin area, supratip area, nose wings, and also shortening of the nostrils' superlative. In this piece of work nosotros do not consider patients with great width in the base, but low in the nasal tip noses, as well as noses that had wide nostrils.
Materials and methods
48 cases of rhinoplasty were analyzed. In these cases we performed excision of skin backlog in accord with our method. We performed this number of surgeries from February, 2003 till May, 2012, which is 8% of all the interventions concerning artful deformations of the nose shape. The age of the patients was ranged from xx to 48 years old. There were 37 women and 11 men.
The patients were divided into 3 groups, based on the divergence in the volume of excess peel removal during the surgeries:
- Patients who needed reduction of peel excess but from the nasal tip that could be attained past its excision in the columella area (xix persons – 39%).
- Patients who needed skin excess reduction separately from the nose tip and separately from the olfactory organ wings (21 persons – 43%).
- Patients who needed total nose skin backlog reduction (8 persons – 18%).
Description of the surgery techniques
Surgery technique for the patients of group I
Regular surgery mark, as for open rhinoplasty (Figure iii). We performed the incision in accordance with the mark: along the cutaneous part of the columella, then forth its lateral surface upwards to the cupula so forth the internal surface of the wing. Nosotros made a like incision on the other side of the nose. We mobilized the cutaneous roofing of the nasal tip and partially of the wings, made surgical manipulations on the osseo-cartilaginous structures, and, in cases of necessity, on the inside of cellulocutaneous flap, hemostasis (Figure iv). Subsequently that we pulled the margins of the flap downwardly to the columella, excised the skin backlog and sutured the edges of the wound using interrupted stitches. Meanwhile, get-go information technology is important to cut the top border of the wound of the columella in iii places - one cut is in the middle part and the two of the others are at the both end (Effigy 4a). The length of the skin cuts depended on the quantity of the cutaneous covering that was supposed to be excised. The cuts bases and the inferior border of the wound were sutured using guiding iterrupted stitches. The peel excisions were made sequentially from the left and correct sides between the sutures, in carve up pieces that had the same shape and size. Then the wound was finally closed.
Figure 3. Presurgical marking on the plaster cast for the patients of group I.

Figure 4. Mobilization of the nasal tip cutaneous roofing.

Figure4a. Dissection of the top border of the columella wound in three places.
Thus, the only difference between this surgery technique and the well-known technique of "open up" rhinoplasty is that we tin can make additional excisions of skin excess in the area of the columella, if necessary.
It is necessary to attract your attending to the fact that the methods of columella skin excision had been offered earlier, but it was recommended in society to ameliorate cicatrix aesthetics after a failed open rhinoplasty [10].
Surgery technique for the patients of group II
The marking and the appropriate surgery were performed according to the technique mentioned above. But we also made classical excisions of semilunar pieces of the skin at the base of the nose wings. The last action was necessary for the length and convexity reduction of the wings (Effigy 5).

6. Figure5. Presurgical mark on the plaster bandage for the patients of group 2.
Surgery technique for the patients of grouping Iii
(please, scout our video).
Marker (Figure 6), and the incision were made in the same way equally during the surgery for the patients of group I, but after the incision was prolonged downwardly forth the interior wing side to its base of operations. We "went" round the front end edge of the base of operations and "came" to the pare surface of the wing forth the lines of the fold. The incision ended in the place where the fold of the wing base of operations concluded, that is at the border of the lateral nasal wall. We made a whole block mobilization of the cutaneous roofing of the necessary size – nasal tip, nose wings, nasal curvation, and lateral nasal walls (Effigy 6a). Also we made surgical manipulations on the osseo-cartilaginous and the other structures, their correction, and hemostasis. In the cases of necessity, we made thinning of cellulocutaneous flap from the internal surface side. After that we pulled the margins of the flap downwards to the columella and laterally to the wings. The excess skin excisions in the columella surface area were made in the same way as during the surgeries for the patients of group I – with a preliminary dissection of the top border of the wound and putting guiding interrupted sutures. The aforementioned dissections and wound closures were made in the cupula area, the wings internal surface area, and also exterior at their base - three-5 pieces on each side (Figure 6b). Skin excisions were fabricated sequentially from the left and right sides between the sutures, in separate pieces that had the same shape and size. And only after that the wound was finally closed (Figure 6c).

Figure6. Presurgical marking on the plaster bandage for the patients of group III.

Figure 6a. Mobilization of the nasal tip cutaneous covering, wings and other parts of the nose.

Figure 6b. Dissection of the pinnacle edge of the wound of the wing.

Figure 6c. Excess skin flaps.
Thus, mail-operative stitches were put in the parts that were typical for open rhinoplasty surgery: in the columella expanse, cupula surface area, nose vestibule area, and also along the folds at the bottom of the wings. That is why the stitches were barely visible (Figures 6d and 6e).

Figure 6d. Postoperative stitches (the photo made in 2 days afterward the surgery).

Figure 6e. The result in 1 year later on the surgery, bottom view.
It should be noted that the direction and dimensions of the incisions, used in this case, and the great length of the flap mobilization did not cause any concern that the flap edges would fall in necrosis. The safety of this approach was demonstrated by our colleagues in their earlier publications [11,12].
Results
The technique of intervention, described to a higher place, was developed especially for excision of a great nose skin excess (patients of group III). The first surgeries were performed precisely in such cases (Figures 7 and 8). Nonetheless, subsequently we noticed that when we performed the surgeries of classical open rhinoplasty sometimes while matching the wound edges on the columella, some peel excess appeared. Our observations showed that those were patients with bigger "pineal" or "duck" nasal tips, who had peel backlog equally a result of cartilaginous base reduction of the nasal tip at the end of the surgery. That is why an idea of backlog skin excision only from the columella area came to our minds. Having performed several of such surgeries (group I), we noticed a positive influence of this technique on the surgery results - the skin on the tip was tightly pressed towards the underlying structures and survived faster (Figures 9 and 10).

Effigy vii. Patient E…, 42 years one-time; she has a big "pineal" nasal tip, a nose with wide rounded wings and thick, porous skin, full face view (group Iii). Before the surgery.

Effigy 7a. See Figure7. In 2 years.

Figure 7b. Run across Figure7, before, profile view.

Figure7c. See Figure7. In 2 years.

Effigy 7d. Plaster casts of patient E's… nose: on the right – before, on the left – in ii years.

Figure8. Patient L…, 24 years one-time, was operated on in some other clinic 1 year ago. His nose is large (tip, wings). He has thick, porous pare – profile view (grouping III).

Figure 8a. See fig eight. In 2 years and 3 months.

Effigy 8b. Meet fig 8. Full face up view.
Figure 8c. Come across fig 8. In two years and 3 months.

Figure 8d. Come across fig 8. Bottom view.

Figure 8e. In 2 years and 3 months.

Effigy 9. Patient I…22 years old. She has a big nasal tip, apparent lateral limbs of wing cartilages, full confront view (group I).

Figure 9a. Run into fig 9. In 1 year and ii months.

Figure 9b. Run across fig 9. Full face view, before the surgery.

Figure 9c. Run across fig ix. In ane year and 2 months.

Effigy ten. Patient R… 20 years old, before the surgery. She has a big "pineal" nasal tip, full face view (group I).

Effigy 10a. See fig 10. In 1 year.

Figure 10b. Come across fig 10. Profile, before the surgery.

Figure 10c. Run across fig ten. In 1 year.
The next stage involved performing of such surgeries of rhinoplasty that required combined excess peel excision in the columella expanse and semilunar flaps of wings base skin (group II). The results of the surgeries performed in the way described above were also expert (Effigy 11).

Figure 11. Patient D…, 26 years old, was operated on in another country. His nose is big (nasal tip, wings). He has a low wide nasal curvation, full face view (group II).

2Figure 11a. Meet fig eleven. In i yr and vi months.

2021 Copyright OAT. All rights reserv Figure 11b. Run across fig 11. Left profile view, before the surgery.

Figure 11c. See fig 11. In 1 twelvemonth and 6 months.

Figure 11d. See fig xi. Left half profile view.

Figure 11e. See fig 11. In i twelvemonth and 6 months.

Figure 11f. See fig 11. Lesser view. In one year and 6 months.
During our practise we often accept had the necessity of nostrils' height and width reduction. Sometimes it was necessary for a ane-side reduction of a nostril. The technique mentioned above immune us to "shorten" nostrils and attain a good effect with cicatrices in barely visible parts of the olfactory organ (Figures 12 and 12a).

Effigy 12. Patient D-a, 29 years onetime. Nose with long rounded wings, big prolonged nostrils, bottom view (group III).
Effigy 12a. See fig 12. Immediately after the surgery.
Give-and-take
Experienced rhinologists decide the presence of nose peel excess even at the offset examination of the patient and prognose its appearance while performing a rhinoplasty surgery. Therefore they decide in advance which technique of intervention to use. They normally have a choice of performing flap excisions of the peel from the nasal arch or from the nasal tip (horizontal, vertical, Figured) or perform only classical rhinoplasty without excess skin excisions and "wait" (ofttimes in vain) for its expanse reduction in the post-operative period. The patient's stance in choosing one of the techniques plays an important role. He/she can pass up both the possibility of getting a post-operative cicatrix in a visible part of the olfactory organ, and the necessity of waiting for a final result during several months. We used to decline such patients and recommended them to accept their aesthetic nose deformation.
The developed technique mentioned to a higher place made it possible for united states of america to solve these problems: as a result we could assist patients with large noses with thick spongy skin. We think that this technique is successful due to the following two factors: a) excision successfulness of the required skin quantity during the operation, b) invisibility or visibility of post-operative cicatrices. At the beginning of this technique testing and after, during feel accumulation, nosotros were completely enlightened that such a technique would non allow the states to brand an exquisite nose shape similar in the cases of noses with thin peel, because the structure, thickness, and skin color of the nose would not change. Just skin area would reduce. Therefore we consider it improper to compare mail service-operative results at rhinomegaly with a thick porous skin and a "Caucasian" olfactory organ with a slight convexity and thin skin.
As in our practice we have never used modifications of rhinoplasty with skin excisions proposed earlier, we cannot show you any comparing of the results with the use of this method and other similar methods. We tin can simply prove ii cases when patients with bigger noses were operated on using classical method of rhinoplasty in other clinics. After a while they were re-operated on in our clinic with the help of our technique. Such cases can evidence how successful our technique is:
Instance one
Patient L.., 24 years quondam, was operated on in some other clinic i year ago. When he came to our dispensary we could notice a big nose, prominent nasal tip, big wings, thick, porous skin, and cicatrix on the columella typical for open rhinoplasty (Figures 8, 8b, 8d). From the anamnesis we could see that his nose had been bigger before the beginning surgery, merely the surgeon had not fabricated it pocket-sized plenty. That is why the patient did not like the result. Nosotros supposed that the previous surgeons had used classical open rhinoplasty without backlog pare excisions. Therefore, while reoperating the patient we used rhinoplasty according to the type III (excess skin excisions in the columella area, in the cupula surface area, in the wings internal and external surfaces area) with a correction of the osseo-cartilaginous base of the olfactory organ. The postoperative period passed without complications. The concluding nose shape satisfied both the patient and the surgeons (Figures 8a, 8c, and 8e).
Case two
Patient D…, 26 years onetime, was operated on in some other land a year and 6 months agone. When he came to our clinic we could notice a big nose with thick porous skin, deformed nasal tip, convex wings, low and wide nasal arch, typical cicatrices at the bottom of the wings of the nose and in the nose antechamber expanse (Figures 9, 9b). Nosotros suppose that those were results of close rhinoplasty with excision of semilunar pieces of peel at the lesser of the wings. In our clinic we used open rhinoplasty: correction of the lateral limbs of the wing cartilages, osseous office of the nasal curvation and lateral surfaces, and also excision of the semilunar of skin areas at the bottom of the wings. During the wound edges accommodation excess skin appeared on the columella. It was excised co-ordinate to our technique. Thus, the surgery was performed according to blazon Ii (Figures 9a, 9c). The last effect was good.
Surgeons in other clinics refused to brand rhinoplasty to well-nigh of our first patients that we operated on according to the technique (group Iii and partially group Two), or did not guarantee a satisfactory outcome due to the skin excess and because their peel was quite thick and porous. That is why after our intervention they were pleased with the consequence. Complications that we were concerned about because of the dimensions of the incisions and peachy length of the flap mobilization did not arise. We did non brand radical resections of cartilages. We also excised a moderate amount of hypodermic soft tissues. Mucosa integrity was not changed. That is why later quite a long period of time of the post-operative period our patients did not take problems with animate in any instance.
Nosotros excised a great amount of skin in the cases of the patients of group III (Figures 6c), moderate amount of skin in the cases of the patients of group 2 and pocket-size quantity of skin in the cases of the patients of grouping I. Skin excisions were performed in such a way that mail-operative cicatrices were left on the skin of the columella, on the folds of the nose wings and intranasally – on the border of the skin and nasal mucosa. The wounds healed over by the primary intention, without hypertrophy and deformation of cicatrices. Therefore nasal passage constriction did not happen.
Conclusion
The described modification of open rhinoplasty can be effective in cases when the prediction of olfactory organ skin reduce during the postoperative period is doubtful (because of the advanced age, thick and porous pare), or initially there is an credible skin backlog, and we know about the necessity of its excising during the surgery. In this example, information technology is possible to plan quite a lot of backlog peel excision, thus, postoperative cicatrices will be left in the barely visible parts of the nose.
This technique likewise tin can be successfully used for correction of noses with big, long or asymmetrical nostrils, for the purpose of making them lower. Obviously, the described modifications of rhinoplasty can be used besides for correction of a "prominent" nose and also for "parrot nib" deformation corrections.
References
- Aiach GC, Kelly MH (2005) Secondary Rhinoplasty. The art of Aesthetic Surgery. Principles and Techniques. Editor: Foad Nachai. Inc. St. Louis, Missouri. 1618-1676.
- Ezrohin VM, Nikitin AA (1996) Surgical methods of correction of the nose with thick porous pare. Russian Rhinology N1. lx-63.
- Fuleihan NS, Webster RC, Smith RC (2008) Deformity of the Nasal Base. Aesthetic Facial Surgery. Editor: Norman Pastorek. Lippincott 289-310.
- Larrabee WF (2008) Rhinoplasty in the Crumbling Patient. Aesthetic Facial Surgery, Editor: Norman Pastorek. Lippincott 361-384.
- Marchac D, Arnaud Due east (2011) Complications in Craniofacial Surgery: How to Care for and to Avoid Them. fourth Congress of Plastic Surgeons of Armenia and fifth of Georgia 22.
- Sulamanidze M, Adamyan A, Sulamanidze G, Sultanova Due north, Nishnianidze K (2002) Simultaneous aesthetic interventions on the face up for rhinoplasty. Annals of Plastic, Reconstructive and Aesthetic Surgery i: 7-twenty.
- Sulamanidze M, Adamyan A, Sulamanidze Grand, Nishnianidze G (2004) Artful surgery of the broad nose. Register of Plastic, Reconstructive and Aesthetic Surgery 3: 6-17.
- Sulamanidze 1000, Adamyan A, Sulamanidze G (2009) Aesthetic Rhinoplasty in Rhinomegaly. Own Experience. xi-thursday ESPRAS Congress. 347.
- Sulamanidze M, Adamyan A, Sulamanidze G, Nishnianidze G (2011) Artful surgery of the broad nose. Our approaches. 34th Annual Conference of the European Academy of Facial Plastic Surgery. p 6 .
- Gryskiewicz JM (2002) The "iatrogenic-hanging columella": preserving columellar profile later on tip retroprojection. Plast Reconstr Surg 110: 272-277. [Crossref]
- Bafaquen SA, Quattan MM (2000) Simultaneous open Rhinoplasty and Alar Bas excision: is there a problem with the claret supply of the nasal tip and columellar skin?. Plast Reconstr Surg 105: 344-347.
- Marino A (1966) Considerazioni Sulla "Rinotomia Esterna Per Via Dissimulata" Goumain East Planes. Il Valsalva XLII: iii-11.
Editorial Data
Editor-in-Chief
Chin-Lung Kuo
Director of the Section of Otolaryngology
Hsinchu Military Hospital, Hsinchu
Taiwan
Article Type
Research Article
Publication history
Received appointment: April 18, 2016
Accepted date: May 22, 2016
Published date: May 27, 2016
Copyright
©2016 Sulamanidze M. This is an open up-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Commendation
Sulamanidze M (2016) How to remove nose skin backlog? Aesthetically reasonable arroyo. Otorhinolaryngol Head Cervix Sur,1: doi: 10.15761/OHNS.1000107
Figure 1. The instance of complications later close rhinoplasty that happened while operating on the patient with a thick, porous skin – shapeless nasal tip, dimension mismatch of the cartilaginous stractures and skin.
Figure two, 2a, 2b. Plaster casts on which you tin see incision marking for excess skin excisions – classical variants.

Figure 3. Presurgical marking on the plaster cast for the patients of group I.
Figure 4. Mobilization of the nasal tip cutaneous covering.
Figure4a. Dissection of the top border of the columella wound in 3 places.
Figure5. Presurgical marking on the plaster cast for the patients of group II.
Figure6. Presurgical marking on the plaster bandage for the patients of group 3.
Figure 6a. Mobilization of the nasal tip cutaneous covering, wings and other parts of the olfactory organ.
Figure 6b. Dissection of the elevation edge of the wound of the fly.
Figure 6c. Backlog peel flaps.
Effigy 6d. Postoperative stitches (the photo made in 2 days subsequently the surgery).
Effigy 6e. The result in 1 yr after the surgery, lesser view.
Effigy vii. Patient Due east…, 42 years old; she has a big "pineal" nasal tip, a olfactory organ with wide rounded wings and thick, porous skin, full face view (group III). Before the surgery.
Figure 7a. See Figure7. In 2 years.
Figure 7b. See Figure7, before, profile view.
Figure7c. See Figure7. In 2 years.
Figure 7d. Plaster casts of patient Due east'southward… nose: on the right – before, on the left – in 2 years.
Figure8. Patient 50…, 24 years old, was operated on in some other clinic i year ago. His nose is big (tip, wings). He has thick, porous peel – contour view (group III).
Figure 8a. See fig 8. In 2 years and 3 months.
Figure 8b. See fig 8. Full face view.
Effigy 8c. Run into fig 8. In 2 years and 3 months.
Figure 8d. Come across fig viii. Bottom view.
Figure 8e. In 2 years and 3 months.
Effigy nine. Patient I…22 years onetime. She has a big nasal tip, apparent lateral limbs of wing cartilages, full face view (grouping I).
Figure 9a. See fig 9. In one year and 2 months.
Figure 9b. Meet fig nine. Total face up view, earlier the surgery.
Figure 9c. See fig nine. In 1 yr and 2 months.
Figure 10. Patient R… 20 years old, before the surgery. She has a large "pineal" nasal tip, full face view (group I).
Effigy 10a. Run across fig 10. In one year.
Figure 10b. See fig x. Profile, before the surgery.
Effigy 10c. See fig ten. In ane yr.
Figure 11. Patient D…, 26 years old, was operated on in some other land. His nose is large (nasal tip, wings). He has a low wide nasal curvation, total face up view (group Ii).
2Figure 11a. See fig eleven. In 1 year and six months.
Figure 11b. See fig 11. Left profile view, before the surgery.
Figure 11c. See fig 11. In 1 year and 6 months.
Effigy 11d. See fig xi. Left half profile view.
Effigy 11e. See fig 11. In 1 twelvemonth and 6 months.
Figure 11f. See fig eleven. Bottom view. In i year and 6 months.
Effigy 12. Patient D-a, 29 years old. Olfactory organ with long rounded wings, big prolonged nostrils, bottom view (group III).
Figure 12a. Run across fig 12. Immediately after the surgery.
Source: https://www.oatext.com/How-to-remove-nose-skin-excess-Aesthetically-reasonable-approach.php
0 Response to "How To Reduce Thick Skin On Nose"
Post a Comment